
The Third Man and the changing role of antibiotics in our society
On a cold Friday night in November more than a hundred people gathered in the John Snow lecture theatre, at the London School of Hygiene and Tropical Medicine (LSHTM), to watch The Third Man, a black and white film set in post World War II Vienna, to discuss how antibiotics changed modern healthcare.
The Third Man, directed by Carol Reed and written by Graham Greene, begins with Holly Martins, a writer of American Westerns, going to Vienna to visit his schoolfriend, Harry Lime. When he arrives he is told that Lime died in a car accident earlier that day. Martins then meets with Lime’s friends, some of whom mention a “third man”, who helped carry the body to the side of the street. Martins considers the death suspicious and begins his own investigation to find this mysterious third man.
Eventually, it is revealed Lime was running a racket; he was buying up military hospital penicillin supplies, diluting them to make the drug stretch further and selling the vials off at a great profit to himself. The substandard penicillin was given to children with meningitis but failed to cure it. Martins is taken to a hospital to see the victims. “The lucky ones died, and the unlucky ones lived and went insane”, says detective Major Calloway, who uncovered the swindle.
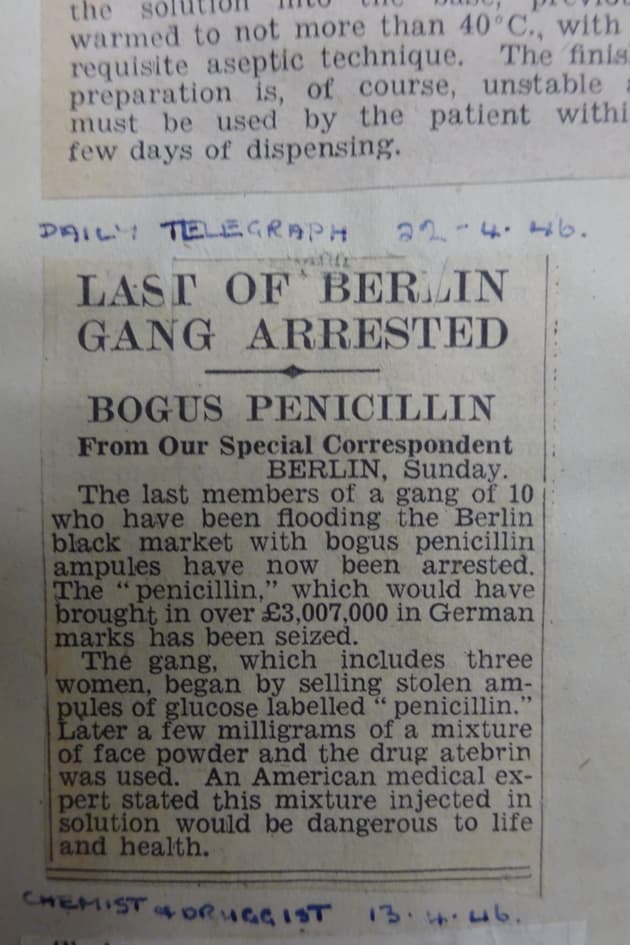 A Daily Telegraph article from 22nd April 1946 describes a fake penicillin racket discovered in Berlin which is thought to have been the inspiration for the film The Third Man
via the Wellcome Trust/Daily Telegraph
A Daily Telegraph article from 22nd April 1946 describes a fake penicillin racket discovered in Berlin which is thought to have been the inspiration for the film The Third Man
via the Wellcome Trust/Daily Telegraph
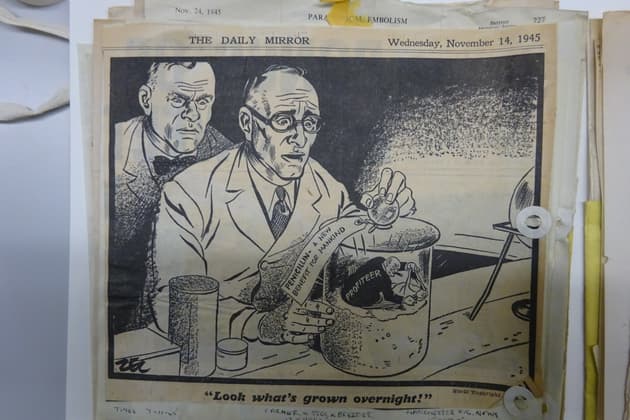 A cartoon published in the Daily Mirror on 14th November 1945, four years after penicillin was first mass produced in the US
via The Wellcome Trust/Daily Mirror
A cartoon published in the Daily Mirror on 14th November 1945, four years after penicillin was first mass produced in the US
via The Wellcome Trust/Daily Mirror
I opened the panel discussion after the film with the observation that substandard antibiotics – which do not contain enough of the drug to kill the infection - don’t help patients get better and can also lead to the development of antibiotic resistant bacteria, or superbugs.
In the West strict regulation means that patients given an antibiotic can be pretty sure it contains the active ingredient advertised at the correct dose. Yet researchers, including those based at LSHTM, have shown that this isn’t the case in many areas of the world. Rackets like Harry Lime’s are still common, with counterfeit, substandard and falsified medicines still a huge problem in parts of Africa and Asia. They also contribute to the global problem of resistance.
Ross Macfarlane, research development lead at the Wellcome Collection, revealed the press cuttings he had unearthed, including articles about a black market penicillin racket in Berlin which is regarded as the film’s main inspiration. Seven men and three women were arrested in 1946 by American and British intelligence service, including a former German army private who was the alleged ringleader, an American doctor and two GIs, American soldiers, in love with young German girls, so-called “frauleins”.
Penicillin had only recently started being mass produced at the time the film was released, and the drugs were seen as innovative. There was a lot of hope they represented the bright future of medicine. Trains advertised antibiotics to the masses – and doctors in Britain were aware of an American invention: penicillin ice cream which soothed throat infections and scarlet fever. Yet even Alexander Fleming, the first scientist to document penicillin, warned of resistance to the drugs in his Nobel Prize speech in 1945.
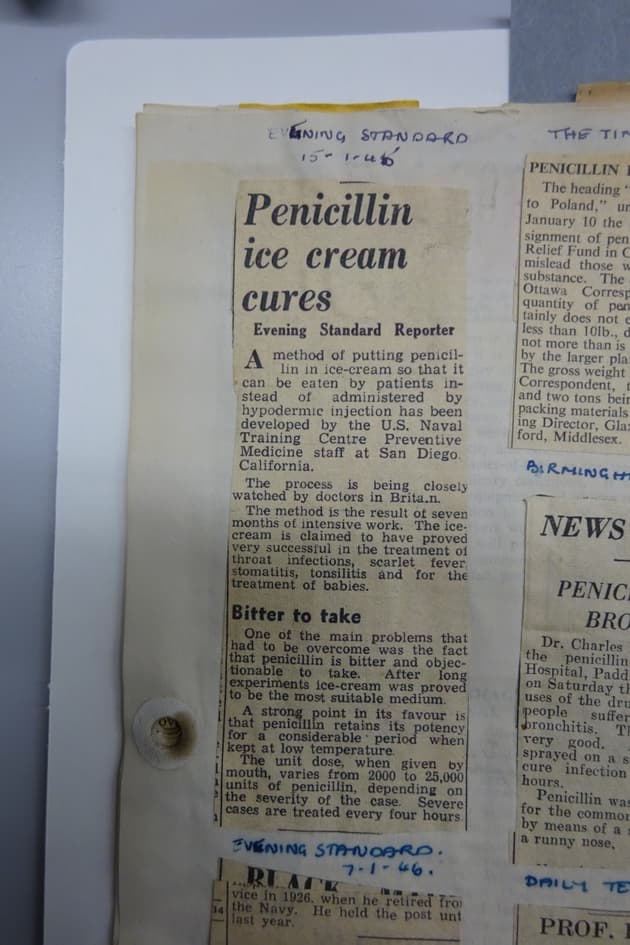 In 1946 British doctors were closely following the invention of penicillin ice cream - a cure for throat infections and scarlet fever among other ailments, an Evening Standard article shows
via the Wellcome Trust
In 1946 British doctors were closely following the invention of penicillin ice cream - a cure for throat infections and scarlet fever among other ailments, an Evening Standard article shows
via the Wellcome Trust
Next, Dr Clare Chandler, a medical anthropologist who co-runs the Antimicrobial Resistance Centre at LSHTM, talked about how antibiotics became more widely used and then triggered changes in healthcare as well as our society. Surgical equipment used to be heavily disinfected to prevent infection, but use of antibiotics before surgery meant hospitals largely stopped doing this. Antibiotics allowed for joint replacements, Caesarean sections and cancer care - the operations we now think of as standard. It also paved the way for factory farming as they could be used as growth promoters. Penicillin, which was a cure for the sexually transmitted infection, syphilis, also lowered the “cost” of casual sex. So it is quite possible that antibiotics, as well as the pill, fuelled the sexual revolution of the 1960s.
Dr Laura Shallcross, a public health doctor and lecturer at University College London, explained how we got to a point where the Government has launched a campaign to reduce antibiotic prescribing. She said no new classes of antibiotics have been brought to market since the 1980s. Meanwhile, global travel means superbugs now spread easily all over the world.
We still don’t have a test which can accurately diagnose whether a patient has a viral illness (in which case antibiotics won’t cure it) or a bacterial one, she pointed out. GPs have reduced antibiotic prescribing, yet they may still prescribe antibiotics when they are not necessary as they come under pressure of “getting it wrong”. Many, if not most mild to moderate infections will actually get better without treatment. Yet when faced with an ill child, doctors do not want to risk an anomaly where a child that does not appear to need antibiotic goes home and dies of a bacterial infection. To prevent this, they will always err on the side of caution.
Questions from the audience included one about whether people should accept that when they are ill they should stay home until they are better and whether this would be accepted by employers. The panel thought that as most people recover from infections without the need for antibiotics, perhaps we do need a societal shift towards patience, rather than pills.
Main picture, of the panel discussion, via the London School of Hygiene and Tropical Medicine.
All images of archive press cuttings were kindly provided by Ross MacFarlane, research development lead at the Wellcome Collection.



